
Why Dental Sealants Sometimes Make Me Nervous
When I see dental sealants on children, I’ll admit it, I often become a little apprehensive about what may be lurking underneath. Not horror-movie apprehensive, but the quiet, professional kind that says, “Hmm… this could go either way.”
More often than I would like to admit, I see children with recurrent decay on their permanent molars hiding beneath worn, chipped, or excessively placed sealants. It’s a bit like lifting a welcome mat off a wooden porch and discovering termites. No one wanted this outcome, yet here we are.
When Dental Sealants Work (And When They Don’t)
Don’t get me wrong, when done properly, dental sealants are an invaluable tool for reducing caries risk, especially in teeth with deep grooves or hard-to-reach anatomy. But like many good things in dentistry, they are technique-sensitive. Without attention to placement and volume, sealants can quietly transition from preventive hero to unintended accomplice.
Case 1: Sealant Breakdown and Recurrent Decay Under Sealants (9-Year-Old Patient)
Patient History
9 year old patient presented for standard recall examination. The patient had dental sealants placed on upper and lower 6’s at a different office when she was 6 years old.
Clinical Findings
Sealant can be seen on both occlusal grooves and up towards cuspal inclines, indicating excess during placement. Sealant margins are no longer smooth, with a dark rim of shadowing seen in certain areas, and others with areas of sealant apparently chipped off.

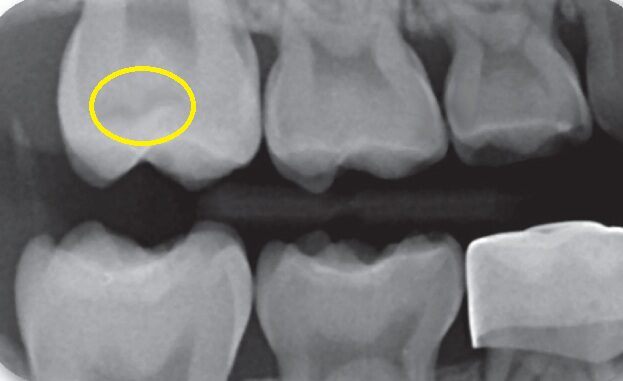
Radiographic Findings
Radiographic bitewing image shows occlusal recurrent caries under the sealants, now requiring further restorative work. It’s a reminder that sealants should live in the grooves, not on the mountain slopes. When bulk increases, so does the risk of wear, fracture, and marginal breakdown, all perfect entry points for bacteria.
Case 2: Minimal Sealant Placement With Long-Term Success (16-Year-Old Patient)
Patient History
16 year old patient presented for standard recall examination. The patient had dental sealants placed on all 6’s when she was 7 years old, and all 7’s when she was 12 years old.
Clinical Findings
Minimal sealant localized just to the deepest grooves on her molars can be seen, with no excess. Marginal seal even on the 6s was still intact and smooth, with no signs of break down or recurrent decay. A case done right!


Dental Sealants Are Most Effective When They Are:
- Placed selectively, only on teeth and surfaces with clear risk
- Confined to pits and fissures, not spread across the occlusal table
- Applied with minimal volume, avoiding bulk and occlusal interference
- Monitored regularly for wear, fracture, or loss
Sealants Are Not a Replacement for Oral Hygiene
Sealants are not a substitute for oral hygiene, fluoride exposure, or dietary control. They are a targeted preventive measure designed to protect anatomy that brushing cannot reliably access.
Final Thoughts: Precision Beats Overbuilding
When placed thoughtfully and conservatively, sealants remain one of the most valuable tools in pediatric preventive care.
When overused or overbuilt, they can undermine the very protection they are intended to provide.
As with many things in dentistry, success lies not in doing more, but in doing it precisely.